
you back again…” (Paul Simon would probably
hate me for repurposing his lyrics like this, even
in jest.)
When a country puts an antivaxxer and supporter of quackery whose worldview with respect to medicine and biomedical science is as utterly divorced from science and reality as that of longtime antivax activist Robert F. Kennedy, Jr. in charge of the nation’s medicine and public health, there are certain predictable outcomes that we can expect to observe over the next few years. The most obvious of these outcomes is the likely return of once-vanquished vaccine-preventable diseases. I was reminded of—and alarmed by!—this likelihood when I came across a modeling study hot off the presses from JAMA last Thursday. The study basically models what might happen as vaccine uptake declines, concluding first that if vaccine uptake declines sufficiently, measles could well become endemic again. (Make measles endemic again? I prefer what I’ve been sarcastically saying about antivaxxers since 2017, namely “Make measles great again.” Because everyone loved the pre-1964, pre-vaccine situation, with millions of cases every year, right?)
Even more alarmingly, though, it’s not just about measles. Measles, being among the most transmissible viruses in existence, is just the canary in the coal mine. It’s come back first, but it won’t be long before other pathogens join it. (Indeed, as I predicted, cases of pertussis—whooping cough—are starting to surge, too.) This study is also about rubella, diphtheria, and even polio. I’ll provide a spoiler alert before I discuss the study in more depth: The model predicts tens of millions of measles cases and millions of polio cases over the next 25 years if vaccine coverage declines sufficiently. (Make polio great again?) It also illustrates how it’s not at all implausible that uptake of various critical vaccines could decline sufficiently to result in this outcome.
Make America Sick
Before I discuss the JAMA study, here’s some obligatory background, with a hint of “I told you so.” (It’s actually more than a hint.) I had started sounding the alarm soon after RFK Jr. bent the knee to Donald Trump last year, suspending his quixotic independent Presidential campaign in return for a prominent role in health policy, which, alarmingly, turned out to be Secretary of Health and Human Services. He’s now in charge of the sprawling bureaucracy responsible for overseeing basically all non-military federal public health and health care policy, including such critical infrastructure as the Centers for Medicare & Medicaid Services (CMS), the Centers for Disease Control and Prevention, the Food and Drug Administration, and the National Institutes of Health. Unsurprisingly, he’s appointed a number of antivax grifters and quacks to head up these agencies. I’m talking “America’s Quack” Dr. Mehmet Oz, who is now in charge of CMS and overseeing Medicare, Medicaid, and the insurance exchanges under the Affordable Care Act. I’m talking Dr. Jay Bhattacharya, co-author of that “let ‘er rip” COVID-19 manifesto (with “focused protection” of the vulnerable as an afterthought) the Great Barrington Declaration, in charge of the NIH. I’m talking COVID-19 contrarian and popularizer of the quack myth that medical errors are the third leading cause of death in the US, Dr. Marty Makary, in charge of the FDA. True, President Trump tried to appoint longtime antivax doctor and politician Dr. Dave Weldon to run the CDC, but that appeared to be a quack too far. (How RFK Jr. himself as HHS Secretary was not a quack too far, I leave as an exercise for our readers.) Unsurprisingly, RFK Jr. set about undermining vaccine programs and, instead of “make America healthy again” (MAHA), we’re seeing him make America sick again.
Of course, RFK Jr. proclaims his MAHA movement as being all about fighting chronic disease and “making America healthy again” by safeguarding the food supply and encouraging healthy eating and lifestyles, thus (if you believe him) leading to a decline in obesity and chronic diseases that he attributes to big agriculture, big pharma, vaccines, and “chemicals.” Indeed, RFK Jr. has made a big show out of a policy to phase out certain food dyes, a move that will almost certainly do little or nothing to “make America healthy again” but sounds good on the surface. I don’t have really have a dog in that hunt and am happy to go where the evidence shows with respect to food dyes, but even the most negative interpretation of the existing data tells me that, even if RFK Jr. is correct about the purported health dangers of these food dyes, eliminating them will have at best marginal effects on public health.
It’s also pretty easy to illustrate just how delusional RFK Jr. is in light of what has happened under RFK Jr.’s watch during the two months he’s been in charge. I will cite some examples. First, you would think that if RFK Jr. were for making America’s children healthy again, he’d be beefing up the CDC’s capacity to deal with known, science-based toxic exposures, like lead, especially given his longstanding fear mongering about mercury in childhood vaccines. Nope. Recently, the health department in Milwaukee asked the CDC for assistance because of a lead contamination problem in its public schools. The CDC declined, because the personnel responsible for such activities had been fired, leading Mike Totoraitis, commissioner of the Milwaukee Health Department, to lament, “April 1 is a really stark moment for public health here across the country, and specifically here in Milwaukee, where now we don’t know who to call. We don’t know how to respond to some of the challenges that we’re dealing with right now because we don’t know if I’m reaching out to someone today, if they’re going to be there tomorrow.” Second, if RFK Jr. were really about protecting the food supply, you’d think that he would have said something about the USDA reversing a Biden-era policy that would have set final standards to determine whether raw poultry products are contaminated with Salmonella, thus moving from a reactive posture to a preventative posture.
Yes, I know that HHS doesn’t control USDA, which is in the Department of Agriculture, but, according to Politico:
Robert F. Kennedy Jr. is fast becoming the most prominent face of the Trump administration’s domestic agenda, taking on a portfolio well beyond the role of a traditional Health secretary. And the White House is thrilled.
And:
Guided largely by his own longstanding fixations on food, wellness and environmental “toxins,” Kennedy is leading a campaign to ban soda and other unhealthy items from the food stamp program, at one point vowing to approve restriction requests sent to “my agency” even though it falls under the USDA’s jurisdiction. A skeptic of fluoridated water, he’s touted the EPA’s reexamination of national fluoride standards.
See what I mean?
Finally, I hearken back to RFK Jr.’s confirmation hearings, when he refused to give a direct answer to a question from Sen. Bernie Sanders asking whether access to healthcare is a human right and countered with a comparison to the right to free speech and an example of the smoker who develops lung cancer:
Free speech doesn’t cost anybody anything, but in health care, if you smoke cigarettes for 20 years and you get cancer you are now taking from the pool. Are you guaranteed the same right?
Yes, you fool. The answer is yes. It’s not just good morality, but it’s good science-based public health, as it’s long been known that one of the key reasons why the US lags behind other wealthy industrialized nations in health outcomes is our lack of universal health insurance, even after the Affordable Care Act. As I said, this was basically “soft eugenics,” “borrowing” a term I heard from the Conspirituality Podcast. However, RFK Jr. is on board with believing that healthcare is not a right, that it’s a privilege. Given that, the proposed elimination of the Substance Abuse and Mental Health Services Administration (SAMHSA), which operates the 988 Suicide and Crisis Lifeline, and the elimination of the Health Resources and Services Administration (HRSA), which is responsible for ensuring access to health care for uninsured, isolated, and vulnerable people (e.g., HIV/AIDS patients, mothers and children, and families in isolated rural communities) start to make sense, even though these are exactly the sort of functions of HHS that work to make America—at least the most vulnerable among us—healthy again. As I have said repeatedly, MAHA is a lot like The Secret combined with the delusion that you have total control over your health, meaning that if you aren’t healthy it’s your fault. Also, let’s not forget the pure neo-Lysenkoism.
If the Politico report is to be believed, RFK Jr. is the most popular cabinet secretary in the Trump administration. Personally, citing the great Charles Pierce’s characterization of Politico as “Tiger Beat on the Potomac,” I’m hoping this is an exaggeration, but it is concerning. RFK Jr.’s purview appears to be expanding well beyond that of a traditional HHS Secretary, and HHS Secretaries have long had a lot of power. One also wonders how RFK Jr. plans to make the FDA and CDC more effective, given the leaked administration draft of its FY2026 budget proposal that includes massive budget cuts for the FDA and CDC:
At many of the health department’s existing agencies, the proposed cuts would deliver a devastating blow. The Centers for Disease Control and Prevention’s budget would be almost halved, from $9.2 billion to $5.2 billion, while the National Institutes of Health would have its funding drop from its current level of almost $48 billion to $27.3 billion.
At the Food and Drug Administration, the budget would also be reduced, from $7.2 billion to $6.5 billion. The memo also proposes that routine inspections of food facilities be contracted out entirely to states, while the Trump administration would take various unspecified actions “so chemicals and other additives in food and food packaging can be expeditiously removed from our food supply.”
I note that the budget cuts to the CDC and NIH would basically destroy the organizations, leaving them shells of themselves, unable to do anywhere near what they do now, and that a massive proposed reorganization included in the budget that would consolidate multiple centers would not save it. If scientists think it’s difficult to get an NIH grant now, if these cuts go through, it will become well-nigh impossible for most scientists. Paylines have long already been so low that less than 10% of grant applications are funded now; look for that payline to plunge into the low single digits. As I have warned before, say goodbye to the greatest engine of biomedical research ever created. As an aside, I did read the proposal and noticed that it actually proposes to eliminate that bastion of quapkademic medicine known as the National Center for Complementary and Integrative Health (NCCIH). That would normally be a good thing, but, given the quackery that infuses MAHA, I strongly suspect that NCCIH would just dissolve into the rest of the NIH, contaminating everything there with its quackery.
As for vaccines, one must concede that the current measles outbreaks didn’t start because of Trump or RFK Jr. Indeed, they can be accounted for easily by declining vaccine uptake during the pandemic, stoked by the antivaccine movement that took the suspicion of COVID-19 vaccines based on their speed of development and novel technology and quickly turned suspicion to fear and generalized that suspicion and fear to other vaccines, regurgitating the oldest antivax tropes in the process and making them mainstream. By the time RFK Jr. was confirmed by the Senate, the west Texas measles outbreak was in full swing and smaller measles outbreaks had popped up in a number of other states. We can, however, blame RFK Jr. for his response since, which has been to downplay the MMR vaccine, grudgingly saying it’s the “most effective” way to stop the spread of measles while promoting all manner of dubious measles treatments, claiming that measles is basically harmless to healthy children without chronic diseases, and seemingly reinforcing the antivax stance of the parents of the two girls who have thus far died of measles during this outbreak. Meanwhile, the NIH is defunding grants supporting the study of mRNA vaccines and studies on vaccine hesitancy, while the FDA is making Novavax jump through the unnecessary hoop of doing another large RCT of its Novavax COVID-19 vaccine before changing its emergency use authorization (EUA) to a full FDA licensure, invoking methodolatry at its most base.
Now, let’s see what could happen if RFK Jr.’s HHS continues to make it harder to approve new vaccines and works to stoke mistrust in the vaccines already approved.
Hello measles, my old friend (and rubella and diphtheria and polio)
So let’s get to the numbers. The study is entitled Modeling Reemergence of Vaccine-Eliminated Infectious Diseases Under Declining Vaccination in the US and coauthored by a multi-institution team lead by corresponding author Nathan C. Lo, MD, PhD at the Division of Infectious Diseases and Geographic Medicine, Stanford University. Given that our current Antivax-curious NIH Director Dr. Jay Bhattacharya hailed from Stanford before his elevation, I find this ironic. In the interests of the “radical transparency” that RFK Jr. claims to espouse even as he shut down FOIA offices of many HHS agencies and gutted the public records office at the CDC, I also note that friend of the blog, pediatrician and vaccine researcher Dr. Peter Hotez, is a coauthor.
The purpose of the study as stated was to “estimate the number of cases and complications in the US under scenarios of declining childhood vaccination for measles, rubella, poliomyelitis, and diphtheria,” and a “simulation model was used to assess the importation and dynamic spread of vaccine-preventable infectious diseases across 50 US states and the District of Columbia.” The idea was to model what the expected results of various vaccination rates would be over a 25 year period using data on area-specific estimates for demography, population immunity, and infectious disease importation risk, one of its inputs being childhood vaccination rates based on 2004-2023 data. The primary outcomes that were modeled included estimated cases of measles, rubella, poliomyelitis, and diphtheria in the US, and the secondary outcomes included estimated rates of infection-related complications (postmeasles neurological sequelae, congenital rubella syndrome, paralytic poliomyelitis, hospitalization, and death) and the probability and timing for an infection to reestablish endemicity.
Endemicity means nothing more than that the disease is continually being transmitted and circulating within a population, unlike the current situation with vaccine-preventable diseases. Because I’m a bit of a geek I’m going to quote a bit about the modeling and the assumptions used:
We simulated the population for each state by using demography and unique population immunity profiles for each infectious disease. For demography, we included 2019 state-specific estimates from the US Census Bureau for birth rate, population size, and age distribution and used state- and age-specific death rates from the National Center for Health Statistics.46 For generation of the age-specific profiles of population immunity, we used a combination of data from the National Immunization Surveys and data reported in published literature (additional information appears in the eAppendix in Supplement 1 and in the Table).25–33 We used state-specific estimates for population immunity (based on available vaccine coverage data from the National Immunization Surveys) for individuals 24 years of age or younger. For individuals older than 25 years of age, we assumed a general US-wide adult population immunity profile for each infectious disease informed by published literature.25–33 These data included seroprevalence estimates or vaccine data for the measles-mumps-rubella vaccine; the diphtheria, tetanus, and pertussis vaccine; and the inactivated poliovirus vaccine.
Each infection had unique pathogen characteristics, including a basic reproduction number, latent period, duration of infectiousness, and risk of complications (Table). Risks of infection-related complications were computed using literature-based risk estimates (ie, fraction of cases with the complication).
To evaluate model validity, we ran the model under current vaccination coverage levels over a 5-year period for each infectious disease. We then compared the estimated case numbers with publicly available observed case numbers reported by the US Centers for Disease Control and Prevention to assess how accurately the model reflects current transmission dynamics (eAppendix in Supplement 1).47
Here’s one of the key “money graphs.” Let me briefly explain. For each disease, the number of cases during the next 25 years was modeled under certain vaccine uptake rates. 0% means no change over vaccine uptake in 2023, while 100% means a 100% decline from 2023 rates; i.e., no children are being vaccinated against that disease. Now, if you look at the graphs, you’ll see a very interesting and disturbing phenomenon:
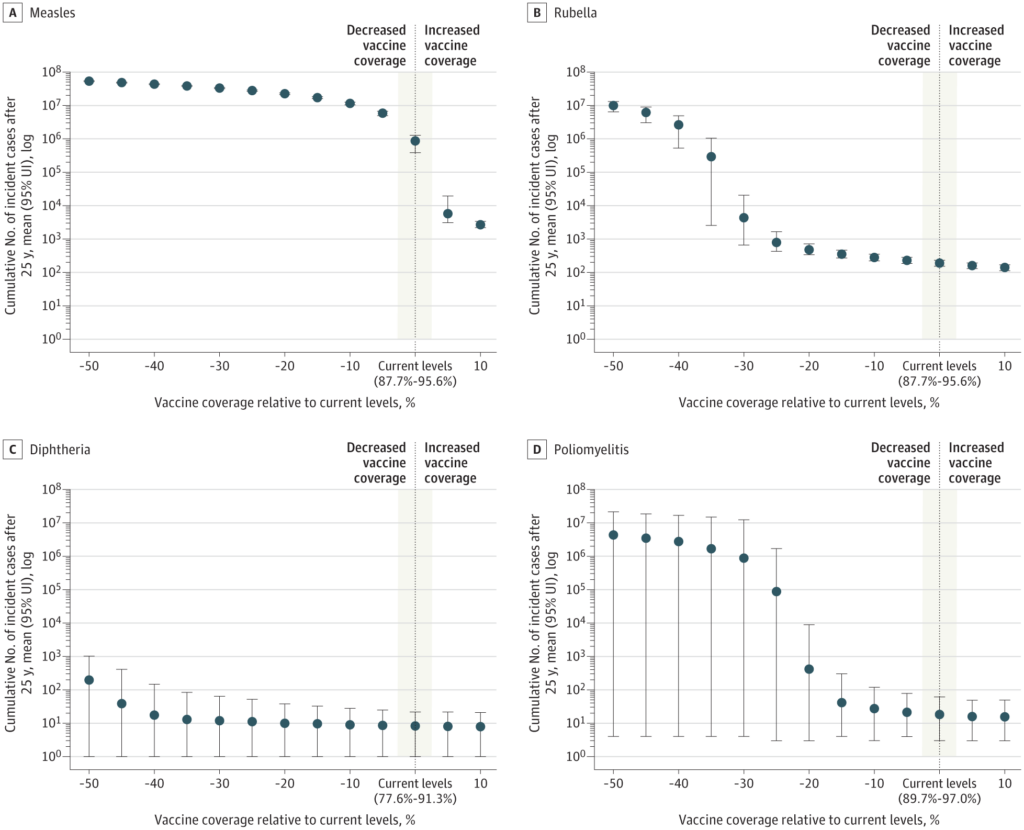
And here is an estimate of complications from these four diseases:
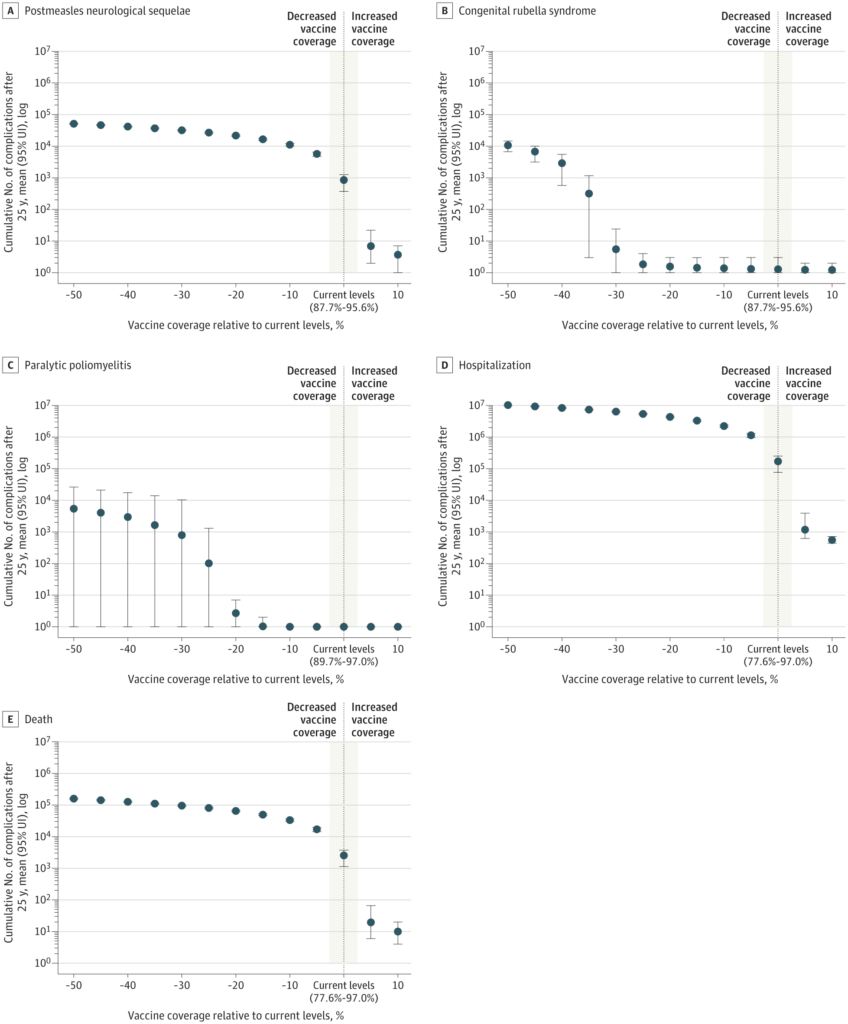
Note, first, that the Y-axes use a logarithmic scale. That means that a 10% decline from current vaccine uptake results in nearly a 10-fold increase in the number of cases of, for example, measles, whereas it takes more like a 25% decline in rubella vaccine uptake to see a ten-fold increase in the number of rubella cases. Alarmingly, a 25% decline in polio vaccine uptake will get us to roughly 100,000 cases of polio. On the other hand, note how increasing measles vaccine uptake by just 10% would result in a dramatic decline of nearly three orders of magnitude.
But what does this mean in raw numbers? The authors estimate first what would happen if current state-level vaccination rates were maintained or improved upon slightly:
Over a 25-year period and under a scenario with current state-level vaccination rates, the simulation model predicted there would be 851 300 cases (95% UI, 381 300-1.3 million cases) of measles, 190 cases (95% UI, 154-230 cases) of rubella, 18 cases (95% UI, 3-61 cases) of poliomyelitis, and 8 cases (95% UI, 1-22 cases) of diphtheria. Under this scenario, we projected 851 cases (95% UI, 372-1270 cases) with postmeasles neurological sequelae, 170 200 hospitalizations (95% UI, 76 200-250 000 hospitalizations), and 2550 deaths (95% UI, 1130-3760 deaths) (Figure 1 and eTable 8 in Supplement 1). Under a scenario with state-level measles-mumps-rubella vaccination rates that were 5% higher over 25 years, there would be 5800 cases (95% UI, 3100-19 400 cases) of measles. With a vaccination rate that was 10% higher, there would be 2700 cases (95% UI, 2200-3400 cases) of measles.
The first thing I noted here is that we are, arguably, already screwed. If nothing changes, we can expect a lot of bad things to happen in the US, at least with respect to measles, a scenario that could be massively improved upon just by a slight increase in vaccination rates, by 5-10%. Of course, this part can’t be blamed on Trump or RFK Jr., at least not directly. I do blame RFK Jr. for his 20 year campaign of promoting fear mongering about mercury in vaccines, MMR vaccines supposedly causing autism, and vaccines (and chemicals) creating what he called the “sickest generation.” Unfortunately, he had a lot of help, particularly during the pandemic. Now that he is HHS Secretary, however, we can see how his promotion of pseudoscientific claims of vaccine harm and his conspiracy theories about vaccines could lead a bad situation to become massively worse. for example:
In contrast, under a scenario with a 10% decline in measles-mumps-rubella vaccination, the model estimates 11.1 million (95% UI, 10.1-12.1 million) cases of measles.
I’d say that, if RFK Jr. is left in charge of HHS for the full four years of the second Trump administration, a 10% decline in vaccine uptake would arguably be a conservative estimate of what is likely to happen. More likely would be a larger decline, such as 25%, which the authors modeled:
If routine childhood vaccination declined by 25%, we estimated 26.9 million (95% UI, 25.5 million-28.1 million) cases of measles would occur within the 25-year period, 790 cases (95% UI, 429-1700 cases) of rubella, 87 600 cases (95% UI, 3 cases to 1.7 million cases) of poliomyelitis, and 11 cases (95% UI, 1-52 cases) of diphtheria. Under this scenario, we projected there would be 26 900 cases (95% UI, 25 500-28 100 cases) of postmeasles neurological sequelae, 100 cases (95% UI, 0-1300 cases) of paralytic poliomyelitis, 1 case (95% UI, 0-3 cases) of congenital rubella syndrome, 5.4 million hospitalizations (95% UI, 5.1-5.6 million hospitalizations) due to all infections, and 80 600 deaths (95% UI, 76 500-84 300 deaths) due to all infections.
Did I read that right? An estimate of nearly 88,000 cases of polio over 25 years? Polio was nearly eradicated worldwide, and RFK Jr.’s policies could well lead to its massive resurgence here in the US. And nearly 81,000 deaths from what are now vaccine-preventable diseases? Is that how RFK Jr. would “make America healthy again”? Apparently so. Maybe he yearns for the days of FDR. And, no, I don’t believe RFK Jr. for a minute when he says he doesn’t want to discourage vaccination or “take away people’s vaccines.” The very best we can expect from him is a not-so-benign neglect, coupled with a failure to promote vaccination. Under such a scenario, I can easily envision vaccine uptake falling by 10-25%, possibly more.
For example, by 50%, which, unless RFK Jr. actually does start delicensing childhood vaccines (which he might, based on his false belief that they cause autism), is unlikely, but worth looking at:
If routine childhood vaccination declined by 50%, the simulation model predicted there would be 51.2 million cases (95% UI, 49.7-52.5 million cases) of measles over a 25-year period, 9.9 million cases (95% UI, 6.4-13.0 million cases) of rubella, 4.3 million cases (95% UI, 4 cases to 21.5 million cases) of poliomyelitis, and 197 cases (95% UI, 1-1000 cases) of diphtheria. Under this scenario, we projected there would be 51 200 cases (95% UI, 49 600-52 600 cases) of postmeasles neurological sequelae, 5400 cases (95% UI, 0-26 500 cases) of paralytic poliomyelitis, 10 700 cases (95% UI, 6700-14 600 cases) of congenital rubella syndrome, 10.3 million hospitalizations (95% UI, 9.9-10.5 million hospitalizations) due to all infections, and 159 200 deaths (95% UI, 151 200-164 700 deaths) due to all infections (Figure 1, Figure 2, and eTables 8-9 in Supplement 1).
In the Supplements, there is a graph that basically shows how many cumulative cases we can expect under various scenarios, including 100% decline, the complete cessation of vaccination:
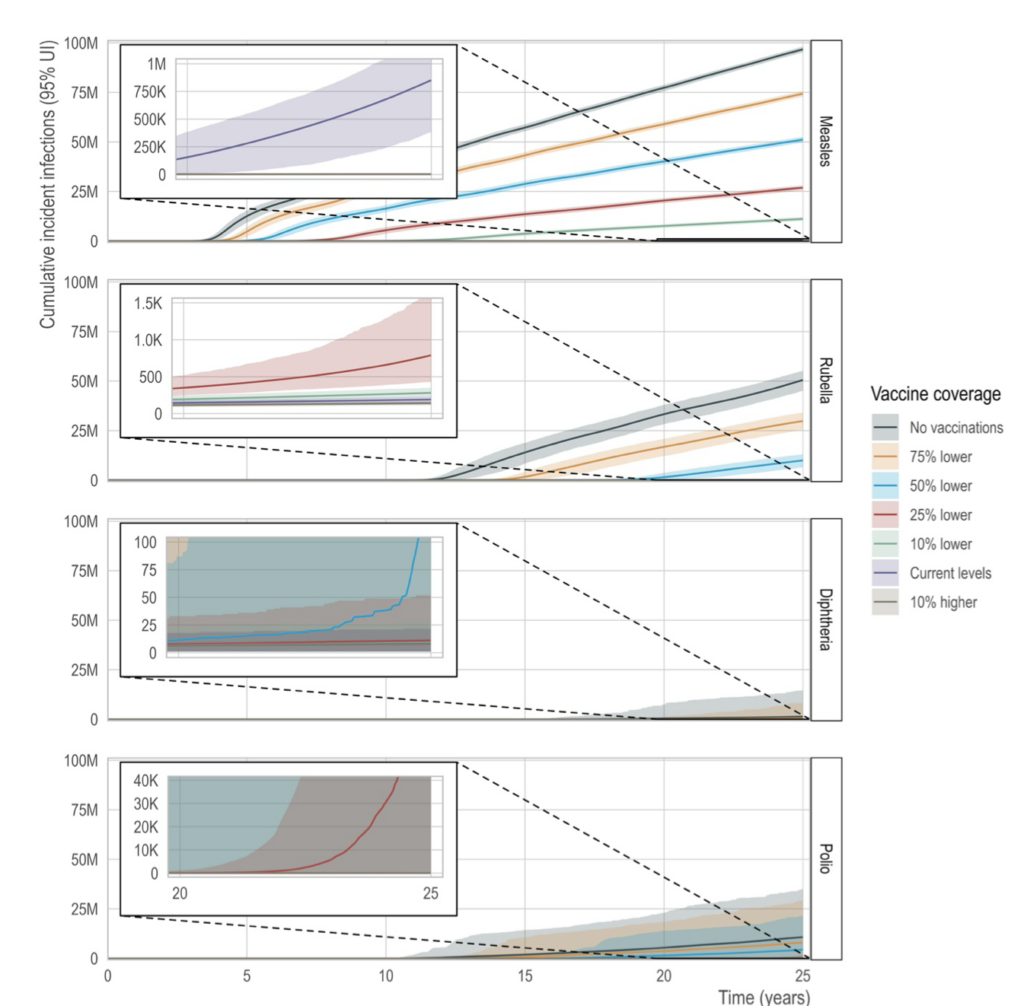
The model estimated mean number of cumulative cases of each disease (rows) under different routine childhood vaccination scenarios (colors), including current state-specific levels of vaccination. Each vaccination scenario is a relative reduced percentage of the current state- specific level of vaccination. The line represents the mean over 2,000 simulations and the shaded region represents the 95th percentile of stochastic uncertainty around the estimate.
And here are the estimated likelihoods of each disease returning to endemicity:
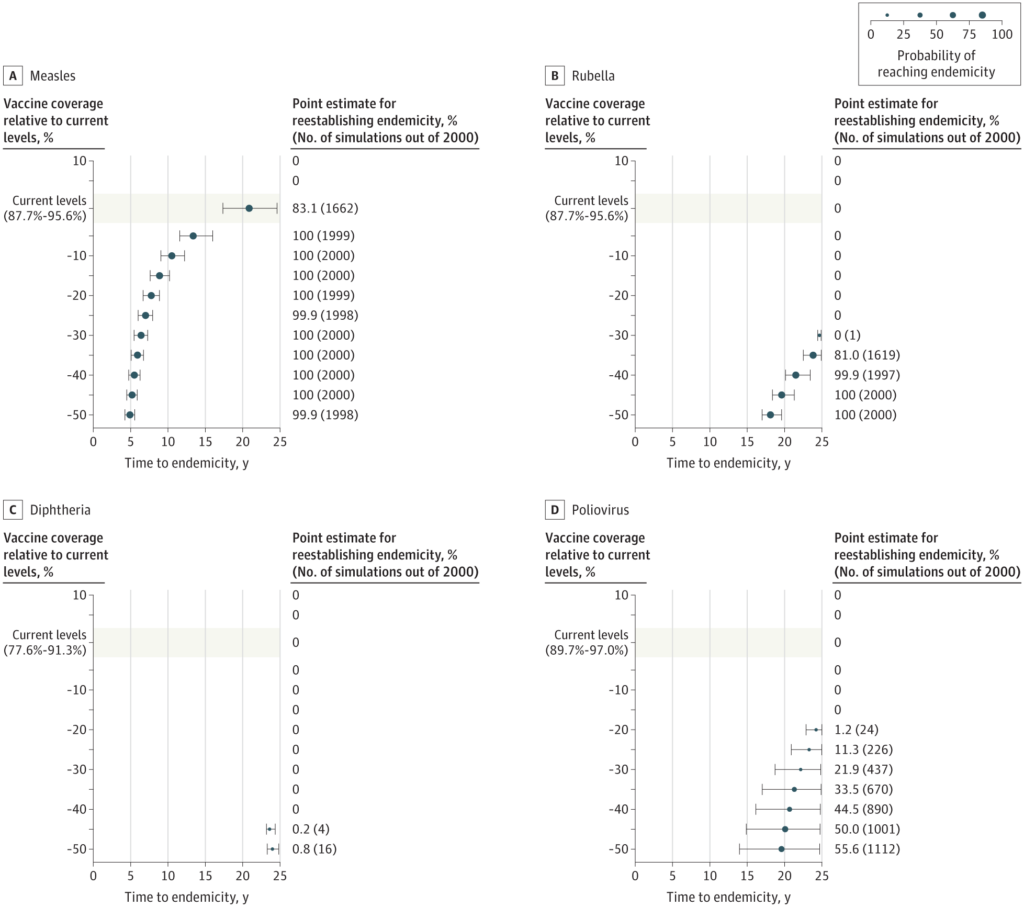
Unsurprisingly, measles, being by far the most transmissible disease, would be expected to have the highest likelihood of becoming endemic again and doing it the fastest. Also, as the authors note, measles is the disease that is most commonly imported from other countries or regions with low vaccine uptake, with polio and diphtheria being the least common.
Like all modeling studies, this one has weaknesses largely based on its dataset and assumptions. For example, some of the assumptions were simplified, although the authors take pains to point out that they tended to use conservative estimates for “model inputs, meaning the risk of outbreaks and speed of reemergence under declining vaccination may be greater than predicted.” Similarly, they modeled outbreaks in states as though the states were independent, when clearly they are not. As we have seen with the west Texas outbreak, measles quickly popped up across the border in New Mexico. As the authors note again, this weakness, if anything, would imply that “the base-case model is an underestimation of total cases given the lack of spillover from state to state.”
Among other weaknesses, this one caught my eye:
Eighth, we did not account for outbreak-related reactive vaccination from public health departments or behavior change on vaccine uptake during outbreaks. Ninth, we did account for age-specific social mixing patterns, but there was homogenous mixing within those groups. However, there may be assortative mixing by vaccine status, which could lead to earlier outbreaks and return to endemicity. We generated mean risk estimates for complications related to each disease, but did not account for age-specific differences in outcomes.
“Assortative mixing by vaccine status.” What they mean is antivaxxers tending to cluster together. In any case, the vast majority of the weaknesses cited by the authors in their model would tend to underestimate, not overestimate, the number of cases expected, with the possible exception of effective reactive vaccination programs from public health departments. Even there, though, I remain pessimistic, because I know that RFK Jr. will not seriously support local public health departments in terms of strong promotion of vaccination campaigns. The states and localities will likely be left on their own.
What can we do?
I hate to be the constant Voice of Doom, but things are bad—and likely to get much worse over the next few years—with respect to public health, medicine, and biomedical research. Because RFK Jr. is gutting the CDC, even if President Trump is replaced by a pro-public health President in the 2028 election, who then appoints a pro-public health HHS Secretary in 2029, it will likely take years, possibly decades, to rebuild the public health infrastructure in the US, and, given the mistrust of public health and vaccines stoked by RFK Jr. (among others) before he was appointed and now being stoked by him as HHS Secretary, who know if there will be the political will to do what it takes to return to a science-based public health and vaccination policy?
It’s not all gloom and doom, even if it mostly is, however:
From the article:
Vaccine scientists and medical leaders announced today they are launching an unprecedented initiative to react to vaccine misinformation and scientifically unfounded vaccine decisions by the U.S. government.
The nascent Vaccine Integrity Project (VIP) is being spearheaded by the Center for Infectious Disease Research and Policy (CIDRAP) at the University of Minnesota and funded by philanthropist Christy Walton, widow of an heir to the Walmart fortune. Led by former chiefs of the National Academy of Medicine (NAM) and the Food and Drug Administration (FDA), next month it will begin to convene leaders across public health and medicine to sound out their views on how to set up such a reaction team, Michael Osterholm, an epidemiologist and director of CIDRAP, told journalists at an embargoed press conference yesterday.
“This project acknowledges the unfortunate reality that the system that we’ve relied on to make vaccine recommendations and to review safety and effectiveness data faces threats,” Osterholm said in a release. At the press conference, Osterholm also referred to August 2024 comments by Jayanta “Jay” Bhattacharya, now director of the National Institutes of Health (NIH), about the technology behind leading COVID-19 vaccines. “Somebody has to be prepared to stand up if the director of the National Institutes of Health declares that mRNA [messenger RNA] vaccine technology is potentially dangerous,” he said.
It’s good that vaccine and public health scientists are pushing back. I wish them luck, even as a nagging voice in the back of my mind asks at the risk of offending or angering allies and colleagues, “Is it too little too late?” After all, the time to push back against misinformation in an organized, effective manner was 20 years ago, when RFK Jr. emerged and first came out as an antivaccine conspiracy theorist and quack. Indeed, I’ll be relieved if the only outright misinformation coming from Dr. Bhattacharya is just that mRNA vaccines are unsafe. After all, he’s already apparently signed on to RFK Jr.’s eugenicist characterization of the “autism tsunami” and endorsed RFK Jr.’s plan to fund dubious research, proposing an autism registry that would mine private medical records, a plan that so alarmed people that HHS backed off on Friday and said there were no plans for such a registry.
Nor do I mean to be too negative. Something needs to be done, and this initiative could conceivably be the spark that gets scientists motivated to push back. As Jason Schwartz says:
Some vaccine advocates not associated with VIP applaud its creation. “It’s important to get such a group up and running and be ready to respond to whatever may come down the line with vaccines,” says Jason Schwartz, a vaccine policy specialist at Yale University. “Because I think we would be kidding ourselves to think there will not continue to be more changes, more threats, more weakening of the federal government’s stewardship of our national vaccination efforts in the months and years to come.”
However the VIP evolves, I’m happy to support it and become involved if there’s anything I can do or if they’ll even have me in spite of my skepticism. More will clearly be needed, however. It’s incredibly difficult for small (thus far) private efforts to counter the tsunami of misinformation and disinformation that is out there now when much of it is now coming from the actual federal government. Contrary to scientists and physicians who sucked up to RFK Jr. because they liked parts of MAHA enough that they thought they could control him, science when it is applied to public policy can’t help but be political. After all, what could be more political than the Trump administration and its MAHA lackey mass canceling NIH grants based not on scientific considerations but on ideological considerations and bullying and punishing universities that do not sufficiently align with its political agenda?
In the meantime, I fear that it’ll be for the foreseeable future, “Hello measles, my old friend.”

{kind=link}